There is a pattern I see in practice with enough consistency that it no longer surprises me. A woman in her mid-to-late 40s describes what she calls a gradual unraveling. Her organizational systems have stopped working. She cannot sustain focus through tasks she managed without effort for years. Her physicians have called it anxiety, burnout, or a consequence of doing too much. Every intervention has failed to fit. Nothing explains it quite right.
What rarely makes it onto the differential is the relationship between her changing hormone levels and a brain that may have always worked differently.
ADHD and Perimenopause at a Glance
Can perimenopause cause ADHD?
No. Perimenopause does not cause ADHD, but hormonal changes can unmask previously compensated symptoms.
Why does ADHD get worse during perimenopause?
Declining estrogen affects dopamine signaling, making attention and executive function more difficult.
Who needs evaluation?
Women whose focus, organization, or emotional regulation changed significantly during their 40s deserve a comprehensive assessment.
What Is the Estrogen-Dopamine Connection?
Estrogen is not only a reproductive hormone. It directly supports dopamine activity in the brain. Dopamine governs attention, motivation, and executive function. ADHD disrupts these same neural pathways.
When estrogen levels are adequate and stable, they help maintain the signaling environment that keeps these pathways functioning. The brain can compensate. Coping strategies work. Many women with undiagnosed ADHD manage reasonably well through their 20s and 30s because their estrogen is doing quiet structural work in the background.
What Changes During Perimenopause
Perimenopause typically begins in the mid-to-late 40s, though it can start earlier. During this transition, estrogen does not decline in a clean, predictable line. It fluctuates, sometimes dramatically, before ultimately declining.
For women with ADHD, whether diagnosed or not, this hormonal volatility disrupts the support system that was already compensating for them. The coping strategies that held everything together for two decades stop working. The experience is often sudden enough that women describe it as an overnight change.
Clinicians misread this clinical picture, regularly and predictably. Anxiety and depression are familiar diagnostic boxes. Attention dysregulation interacting with hormonal transition is not.
The Diagnosis Gap
Research from the Journal of Child Psychology and Psychiatry documents that women wait nearly four years longer than men to receive an ADHD diagnosis, despite being in contact with the mental health system throughout that period. (Skoglund C et al., J Child Psychol Psychiatry. 2023;64(3).)
That gap is not random. ADHD in women more often presents as internal dysregulation, perfectionism, and emotional difficulty rather than the hyperactive and disruptive behavior historically associated with diagnosis. Add the hormonal disruption of perimenopause, and the picture becomes further obscured. Standard care cannot trace this kind of layered history in a 15-minute visit.
The Cardiovascular Layer
If a physician identifies ADHD in midlife and considers stimulant medication, a cardiovascular layer demands active management. Stimulant medications carry real cardiac considerations, including blood pressure and heart rate monitoring over time.
Managing this well means having a primary care physician coordinating across systems, not one who refers and considers the case closed. That coordination is what makes primary care primary. It is also the part that most often falls through the cracks in fee-for-service medicine.
What I Hear in Practice
The hardest thing I hear from accomplished women is not that they cannot get a diagnosis. It is that they did not think they deserved to spend money on themselves. That they explained away years of cognitive and emotional difficulty as personal failure.
If your focus changed in your 40s and the standard explanations have not quite fit, that timeline deserves a proper clinical look. Not because an article can diagnose you. Because you deserve a physician with enough time to investigate.
Frequently Asked Questions
Can perimenopause cause ADHD?
Perimenopause does not cause ADHD.
ADHD is a neurodevelopmental condition present from childhood. However, the decline in estrogen during perimenopause disrupts dopamine signaling, which can unmask previously undiagnosed ADHD or significantly worsen existing symptoms that were manageable before.
Why do women with ADHD get diagnosed later than men?
Research shows women wait nearly four years longer than men for an ADHD diagnosis despite consistent contact with the mental health system. ADHD in women more commonly presents as internalized dysregulation, organizational difficulty, and emotional sensitivity rather than the hyperactive behavior more associated with male presentations. Physicians frequently misattribute these symptoms to anxiety or depression.
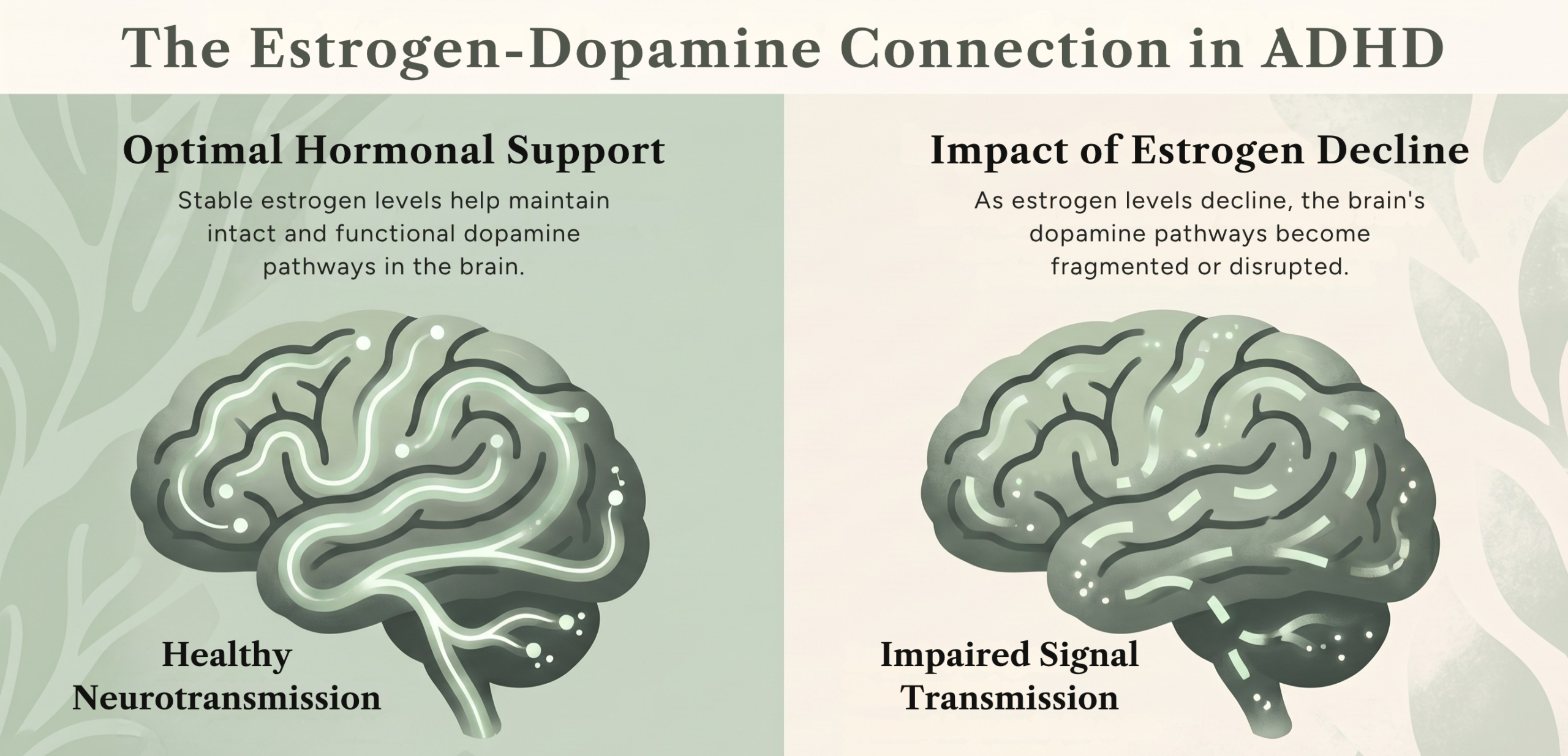
What is the connection between estrogen and dopamine?
Estrogen directly supports dopamine activity in the brain. When estrogen levels decline during perimenopause, the brain’s dopamine pathways lose structural support. For women with ADHD, this makes compensatory strategies significantly less effective.
What should I do if I think my ADHD symptoms are worsening in perimenopause?
The most useful first step is finding a primary care physician with time for a full hormonal and cognitive history, who can trace the timeline of symptom changes, and who will coordinate care rather than refer and close the file. A standard 15-minute appointment cannot do this adequately.
If you’re in the Bethesda area and looking for a more thoughtful approach to primary care, you can schedule a discovery call at BethesdaDoctor.com/contact/. Calls are15 minutes. No paperwork. Just a conversation.
Reference:
Skoglund C et al. J Child Psychol Psychiatry. 2024;65(6):832-44. doi:10.1111/jcpp.13920
Osianlis E et al. ADHD and Sex Hormones in Females: A Systematic Review. 2025. doi:10.1177/10870547251332319
FDA. Safety Review Update: Medications for ADHD in Adults. 2013. fda.gov